
Information
"Information" in the sense of this framework generally refers to data that provide decision-makers with feedback on the program or project. Such information is useful to confirm that an activity is progressing on course or to identify weaknesses in need of mid-course corrections. It also serves as a basis for forecasting future needs in contraceptive commodities.
Information on FP programs in countries worldwide falls into one of three categories:
- Service Statistics
(Routine health information systems including program statistics, client data, and data on sales or distribution of contraceptive products.) - Special studies
- Population based surveys that measure contraceptive use (e.g, DHS, MICS)
Information is the "raw material" for any type of monitoring and
evaluation (M&E) system. The data are often reported in the
form of indicators, which governments, program personnel, and
donors use to track progress.
SERVICE STATISTICS
Public Sector
The Ministry of Health has established the Système National
d'Informations Sanitaires (SNIS, the National System of Health
Information), which covers the full range of health programs in operation
in the country. Specialized health programs, such as the Programme
National de Santé de la Reproduction (PNSR) and the Programme
National de Lutte contre le Paludisme (PNLP, National Program to Combat
Malaria), are expected to feed data from their programs in health
zones throughout the country into the SNIS. Although designed as a national system,
it yields data from approximately one-quarter of the 515 health zones in the DRC.
Système National d'Informations Sanitaires reports on indicators over a wide range of diseases and health topics. The two FP indicators reported in the 2010 annual report were contraceptive prevalence and couple-years of protection (explained below).
NGO Programs
NGOs generally track FP service statistics required by their donors.
Since the Demographic and Health Surveys (DHS) are only conducted
every five years, USAID uses estimates of couple years of protection (CYP)
as an indicator of progress of its programs. Some NGOs also
report on number of new and continuing acceptors.
The services statistics for NGOs may be reported through two channels. First, a given project will report its statistics, such as number of CYP achieved, to its donor. Second, the health zone supported by the project may report these same statistics through the SNIS. This is not problematic unless one combines the CYP achievement reported by the donors and by the SNIS.
Shortcomings in Service Statistics
In its Annual Report 2010, the PNSR lists the following deficiencies related to an information system for FP/RH:
- Insufficient supervision, monitoring and evaluation of RH activities at all levels
- Inadequate capacity to manage RH data characterized by:
- Low capacity to process, use, and disseminate data
- Low capacity to deliver complete information in a
timely fashion - Lack of hardware for data management
- Absence of a base data for RH
- Lack of trained staff in data management for RH
- Lack of a system to verify and consolidate RH data
Five Family Planning Indicators Based on Service Statistics
The five most widely used indicators of FP achievement include the following:

1. Contraceptive Prevalence (Estimated From Service Statistics)
- Definition: the percentage of women in union 15-49 using a contraceptive method
- Method used to calculate it:
- Numerator: number of new and continuing users recorded by program
- Denominator: estimated number of women 15-49 in the catchment area
- Potential biases or limitations:
- Potential errors in reporting the number of new and continuing users
- Inexact nature of the estimate of women in the catchment area
- Missing data from non-reporting health zones: the denominator is not adjusted to remove the population of the non-reporting health zones
- Confusion that "contraceptive prevalence" estimated in this fashion is as robust a measure as contraceptive prevalence measured in a DHS
Couple-Years of Protection Conversion Factors
| Method | CYP Per Unit |
|---|---|
| Copper-T 380-A IUD | 4.6 CYP per IUD inserted
3.3 for 5 year IUD e.g. LNG-IUS |
| 3 year implant (e.g. Implanon) | 2.5 CYP per implant |
| 4 year implant (e.g. Sino-Implant) | 3.2 CYP per implant |
| 5 year implant (e.g. Jadelle) | 3.8 CYP per implant |
| Emergency Contraception | 20 doses per CYP |
| Fertility Awareness Methods | 1.5 CYP per trained adopter |
| Standard Days Method | 1.5 CYP per trained adopter |
| LAM | 4 active users per CYP
or .25 CYP per user |
| *Sterilization: Global
*Sterilization: India, Nepal, Bangladesh |
10
13 |
| Oral Contraceptives | 15 cycles per CYP |
| Condoms (Male and Female) | 120 units per CYP |
| Vaginal Foaming Tablets | 120 units per CYP |
| Depo Provera (DMPA) Injectable | 4 doses per CYP |
| Noristerat (NET-En) Injectable | 6 doses per CYP |
| Cyclofem Monthly Injectable | 13 doses per CYP |
| Monthly Vaginal Ring/Patch | 15 units per CYP |
*The CYP conversion factor for sterilization varies because it depends on when the sterilization is performed in the reproductive life of the individual. For more specific data on CYPs and sterilization, consult with national DHS and CDC reproductive health survey records which may provide a historical calculation based on a specific country’s context.
2. Couple-Years of Protection (CYP)
- Definition: an estimate of the number of couples protected against pregnancy during a one-year period, based on the volume of contraception delivered through the program
- Measurement:
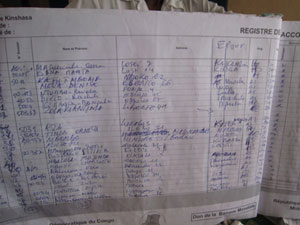
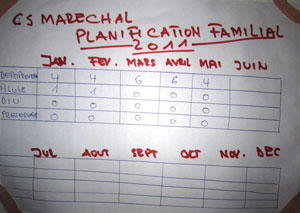
- For a given health zone (or program), one obtains the number of each type of contraceptive sold or distributed free of charge for a specific period (e.g., one month). This information is available from clinic registers and is sometimes posted on the walls of a facility.
- For each contraceptive method, one multiples the number of this method distributed in a given month by a conversion factor, reflecting the length of protection provided by the specific method.
- One sums this amount (number of each type of contraceptive x conversion factor) for each contraceptive to obtain an estimate for the CYP for that zone (or program) for one month.
- One sums the CYP for each month to obtain the CYP equal to 12 months (one year).
- Potential biases or limitations:
- Inaccurate reporting of the volume of contraceptives distributed in each program, facility or health zone
- Errors in applying the conversation factors to arrive at CYP
- Lack of understanding, even among FP personnel, as to what CYP actually measures
- Sometimes based on contraceptive distribution and not use
- Lack of consistency in reporting
3. New Acceptors
- Definition: number of clients (generally women) that accept a family planning method for the first time
- Measurement:
- Based on self-report of women receiving FP services
- Potential biases and limitations:
- There may be inconsistencies in what constitutes a
"new" acceptor: is she "new" if she has received contraceptives at
another time from a different facility? Is she "new" if she comes back after a lapse of time, for example, two years after the birth of a child?
- There may be inconsistencies in what constitutes a
"new" acceptor: is she "new" if she has received contraceptives at
4. Continuing Users
- Definition: the number of clients (generally women) returning to receive services from a given FP site
- Measurement: based on self-report of the clients receiving services
- Potential biases and limitations:
- Programs often use the number of visits of continuing clients to measure number of continuing users; however, if a given client returns 3 times in one year, the program may count this as "3" whereas the person represents "1" returning user. Thus, the number of continuing users is often inadvertently inflated.
5. Disability-Adjusted Life Years (DALYs)
- Rationale: certain social marketing organizations convey the volume of contraceptives sold to couple-years of protection and to DALYs as a rough estimate of the health impact of their programs
- Definition: the number of years of healthy life lost
- Measurement: calculated as the sum of the Years of Life Lost (YLL) due to premature mortality in the population and the Years Lost due to Disability (YLD) for incident cases of the health condition
- Potential Biases and Limitations:
- The implications of age-weighting and discounting are found to be unacceptable.
- There are problems with restricting the framework of health sector analysis and resource allocation to health interventions alone.
Of these five indicators, CYP is most likely to be accurately reported. However, it is not readily understood by health professionals or laypersons outside of family planning.
SPECIAL STUDIES
Some programs conduct different types of applied research to guide the design of new initiatives or to assess the performance of their ongoing programs. These studies may include needs assessment, formative audience research, process evaluation, operations research, and outcomes/impact research, among others. They are called "special studies" because they do not use routinely collected service statistics.
Examples of Special Studies Conducted on Family Planning in the DRC Include:

POPULATION BASED SURVEYS OF CONTRACEPTIVE USE
Two large-scale population-based surveys have measured contraceptive prevalence, related contraceptive behavior, and many other health-related topics in the DRC in recent years:
1. The Demographic and Health Survey
Conducted in 2007, the DHS represents the first nationally representative health survey in the DRC. It provides data on the various topics related to family planning, including the percentage of women that:
- Know a contraceptive method.
- Have ever used a contraceptive method.
- Are currently using a contraceptive prevalence ("contraceptive prevalence rate").
- Are using different types of contraception ("method mix").
- Intend to use contraception in the future (among non-users).
- Have an unmet need for family planning.
The DHS also collects data on fertility behaviors and preferences that affect contraceptive use, as well as reasons for non-use.
The full report is available at:

Please click here for DHS findings on contraceptive use in the DRC
2. The Multiple Indicator Cluster Survey (MICS)
The Multiple Indicator Cluster Survey (MICS), an international
household survey developed by UNICEF, was recently conducted
for the third time in the DRC in 2010. The information
contained in the DRC MICS-2010 covers multiple topics on
households, women, and children. MICS-2 (2001) and MICS-3
(2010) provided family planning data, including contraceptive
prevalence and unmet need.
The MICS also includes data on fertility levels that affect contraceptive use, as well as differences between groups based on background characteristics.
The full report of the DRC MICS 2010 is available at:
The National Institute of Statistics, 6th Street, No.
12, Kinshasa/ Limete- Industrial.
The Ministry of Planning,
Direction des Secteurs Sociaux, 4155, rue des Coteaux,
Quartier Petit Pont, Kinshasa/ Gombe.
The UNICEF office
in the DRC, 87 Boulevard du 30 Juin, Kinshasa/Gombe.
Les résultats préliminaires de l'enquête sont disponibles ici:
 Institut National de la Statistique et Fonds des Nations Unies
pour l'Enfance, Enquete par Grappes a Indicateurs Multiples en
Republique Democratique du Congo, 2010, Rapport de Synthese, Mai 2011.
Institut National de la Statistique et Fonds des Nations Unies
pour l'Enfance, Enquete par Grappes a Indicateurs Multiples en
Republique Democratique du Congo, 2010, Rapport de Synthese, Mai 2011.
Please click here for MICS findings on contraceptive use in the DRC